Pharma B2B: A 2026 Playbook for Compliant, Personalized HCP Engagement in India
Estimated reading time: ~8 minutes
Key Takeaways
- Generic webinars are losing attention; omni-personal 3–6 minute video modules drive relevance and retention.
- Compliance is non-negotiable: align with UCPMP 2024 and DPDPA 2023 using consent-first flows, audit trails, and watermarking.
- Personalization should use HCP attributes, behavior, and context to trigger timely, on-label content.
- Optimize for India: mobile-first formats, burned-in captions, regional languages, and low-latency delivery on WhatsApp.
- Measure clinical intent (qualified completion, CTA conversion) and start with a focused 90-day pilot; leverage Studio by TrueFan AI for compliant automation.
Doctors are ghosting your webinars. It’s not a lack of interest in the science; they simply don't have 45 minutes to spare for a generic slide deck. In the 2026 landscape of pharma B2B engagement, the "one-size-fits-all" broadcast is effectively dead.
The Indian healthcare market has reached a tipping point. On one side, Healthcare Professionals (HCPs) are more digitally savvy than ever but suffer from chronic "Zoom fatigue." On the other, the UCPMP 2024 guidelines and the DPDPA 2023 have turned traditional marketing into a legal minefield.
To win in 2026, you have to stop broadcasting and start narrowcasting. The goal is "omni-personal" engagement: delivering specific clinical insights, in the right language, to the right specialist, at the exact moment they need it—all while keeping your legal team happy.
Why generic videos are failing the "Access Test"
The "access reset" in India is a permanent shift. Post-pandemic, the window for a medical representative to capture a doctor’s attention has shrunk to seconds. Sending the same 20-minute video to a cardiologist in Mumbai and a general practitioner in rural Bihar isn't efficient; it’s an invitation to be ignored.
Indegene’s 2025 trends report confirms that HCPs now demand modular, bite-sized content. They want to see what is relevant to their specific patient profile, not a broad therapy area overview.
Long-form webinars are seeing a 60% drop-off rate within the first three minutes. If your core message is at the 10-minute mark, 90% of your audience will never see it.
The problem isn't the video format; it's the lack of relevance. A resident doctor might need a refresher on the Mechanism of Action (MOA), while a senior consultant is looking for Phase III head-to-head trial data. Serve the same video to both, and you lose both.
In 2026, successful video marketing in India requires a shift toward 3-to-6-minute on-demand modules. These aren't just shorter; they are smarter.
Staying compliant under UCPMP 2024 and DPDPA 2023
This is the primary friction point for pharma marketers: How do you personalize content without violating the "no inducements" rule of UCPMP 2024 or the "explicit consent" requirements of DPDPA 2023?
The UCPMP 2024 code is explicit: promotional materials must be truthful, balanced, and verifiable. Personalization cannot be used to obscure side effects or exaggerate benefits.
Every personalized video variant must be anchored to an MLR-approved "master block." Personalize the greeting, the language, and the case study, but never the core safety data or approved indications.
Then there’s the data. The Digital Personal Data Protection Act (DPDPA) means you cannot track a doctor’s viewing habits simply because they are on your mailing list. You need explicit, purpose-specific consent.
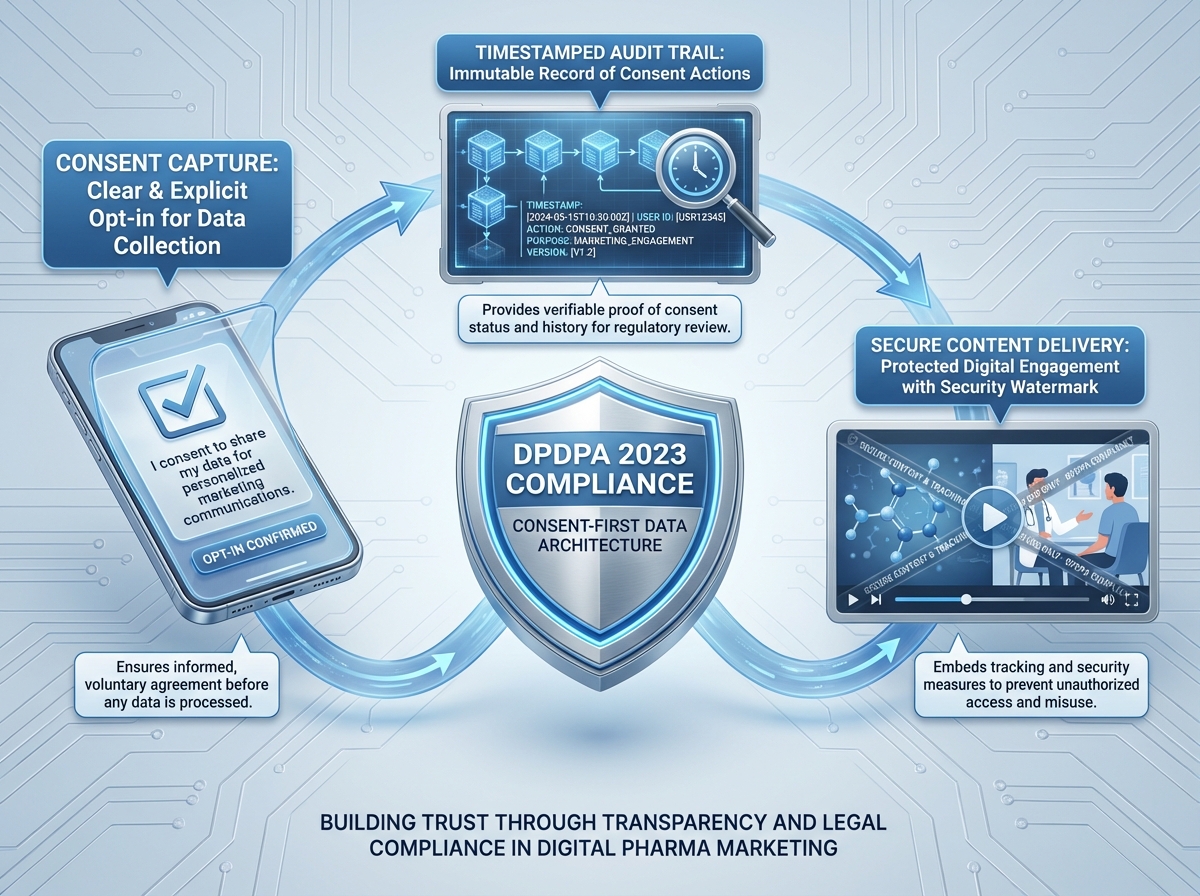
A "consent-first" architecture is now mandatory. This involves:
- Embedded Consent: Video landing pages (on WhatsApp or email) must feature a clear opt-in explaining why you are tracking engagement.
- Audit Trails: A timestamped log of every consent given and every video variant served.
- Watermarking: To prevent unauthorized sharing or "deepfake" concerns, every video should be watermarked with the recipient's ID.
Studio by TrueFan AI manages this through a consent-first model that integrates with your CRM, ensuring no video is generated or sent unless the proper DPDPA-compliant permissions are logged.
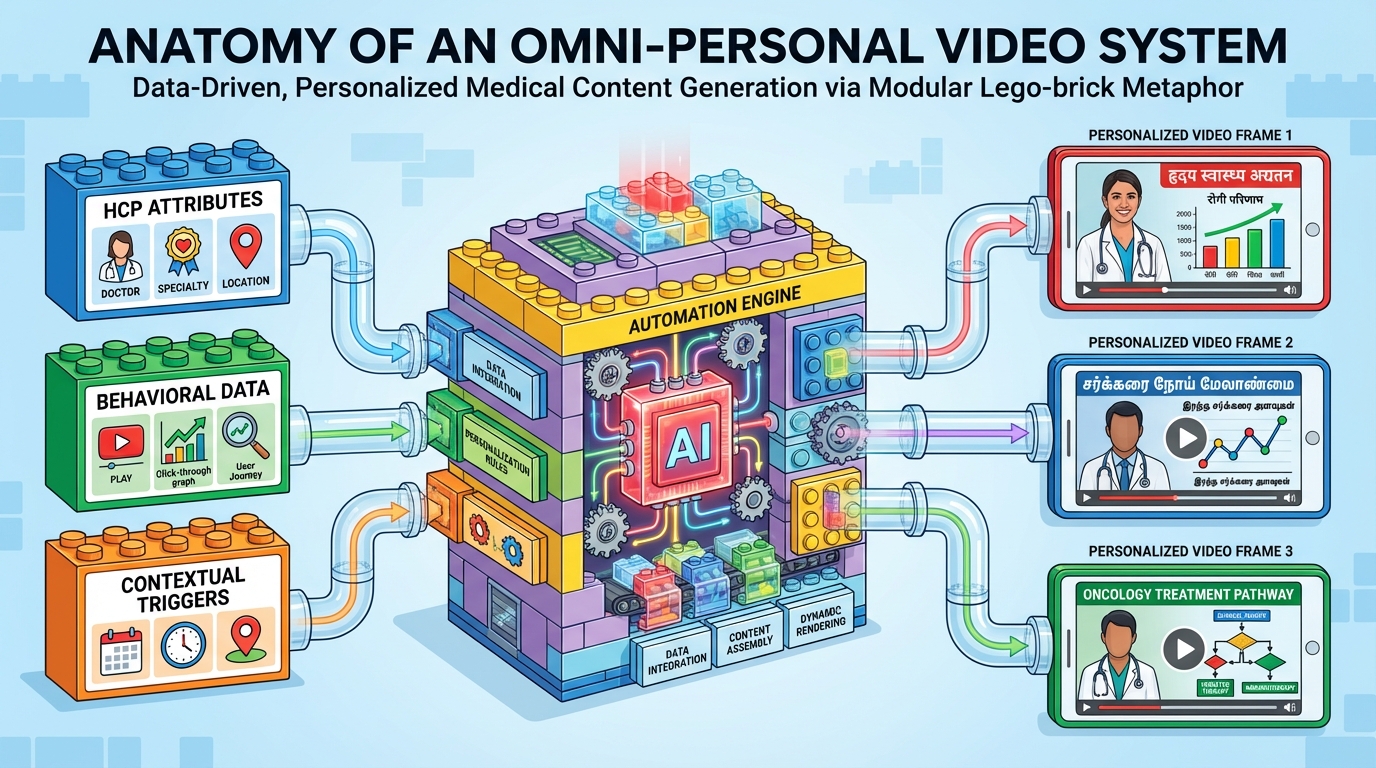
The anatomy of an "omni-personal" video system
Think of this as a Lego set for clinical data. Instead of filming one long movie, you build modules.
A modern doctor relationship personalization platform relies on three inputs:
- HCP Attributes: Specialty, tier (KOL vs. high-prescriber), geography, and preferred language (Hindi, Tamil, Telugu, etc.).
- Behavioral Data: What did they watch last? Did they click "Request MSL" or "Download Monograph"?
- Contextual Triggers: Did they just attend a conference? Is there a new formulary update in their hospital?
When these inputs hit an automation engine, the result is a video that feels bespoke.
Imagine a cardiologist in Chennai receiving a WhatsApp message. The video opens: "Hello Dr. Subramanian, following our discussion on SGLT2 inhibitors at the CSI conference, here is a 3-minute breakdown of the latest renal safety data specifically for your diabetic patients with Stage 3 CKD."
The voiceover is in Tamil. The captions are clear. The data is on-label. That isn't marketing; it's a clinical service.
Use APIs to trigger these videos. When a rep logs a "Call Completed" in the CRM, the system should automatically generate and send a personalized summary video within 15 minutes.
High-impact use cases for 2026
Focus on the moments where personalized content actually shifts behavior.
1. Medical device launch campaigns
Devices require tactile training. In 2026, a manual isn't enough. You send a personalized "OR Setup" video.
- The Video: A 4-minute module showing device setup specific to the hospital’s existing equipment.
- The Personalization: The nurse’s name, the specific model purchased, and local language troubleshooting.
- The Goal: Reduce "time to first use" and minimize user error.
2. Clinical trial recruitment
Recruiting investigators and patients in India is a logistical challenge.
- The Video: Two tracks. One for the investigator (protocol clarity) and one for the patient (rights and "what to expect" visuals).
- The Personalization: Language is critical. A patient in West Bengal needs the explainer in Bengali to provide truly informed consent under DPDPA.
- The Goal: Faster site activation and higher patient retention.
3. Medical conference follow-up
Pharma spends millions on booths, then follows up with a generic "Thank you" email. It’s a wasted opportunity.
- The Video: A 3-minute recap of the specific session the doctor attended.
- The Personalization: "Dr. Kapoor, you attended the session on Heart Failure. Here are the three key slides you saw."
- The Goal: Convert conference interest into a scheduled MSL meeting.
4. Medical rep enablement
The rep remains the vital link, but they need better tools.
- The Video: A post-call summary. Instead of a brochure, the rep sends a 2-minute video recapping the specific patient profile discussed.
- The Personalization: Mentioning the specific clinic and patient type (e.g., "elderly hypertensive patients").
- The Goal: Increase the "second meeting" rate by 25%.
5. Pharmaceutical education automation
Build a library of MOA and safety modules. Use Studio by TrueFan AI to swap the "intro" and "outro" based on specialty. A pediatrician gets a different "patient selection" module than a GP, even if the drug is the same.
Format standards for the Indian market
If your video doesn't work on a mid-range Android phone over a spotty 4G connection in a hospital basement, it’s useless.
- Duration: 3 to 6 minutes. If the topic is complex, break it into chapters.
- Mobile-First: Use 9:16 (vertical) or 1:1 (square) aspect ratios. Doctors watch these on WhatsApp between consultations.
- Captions: Burn them in. Many doctors watch on mute in public spaces or clinics.
- Language: Don't default to English. Indegene's report on digitally-savvy HCPs shows that trust increases when clinical data is summarized in the doctor's primary tongue.
- Clinical Clarity: Avoid flashy transitions. Use high-contrast typography for data. Always include the mandatory "Risk and Safety" slide for at least 5 seconds.
Never use superlatives like "The best" or "The most effective" in your video scripts. UCPMP 2024 auditors look for these "red flag" words to issue notices.
Measuring ROI: From "Views" to "Clinical Intent"
In 2026, we measure intent, not just impressions.
Key metrics include:
- Verified Opens: Did the targeted HCP actually open the link?
- Qualified Completion: Did they watch at least 70%? (The threshold for message absorption).
- CTA Conversion: Did they click "Request Sample" or "Book MSL"?
- Prescription Influence: By tying completion data to CRM records, you can model the impact on specific territories.
Everest Group’s 2025 assessment notes that leaders are now using AI-driven analytics to link content engagement directly to "Next Best Action" (NBA) triggers for reps.
The 90-Day Pilot: A practical start
Don't try to overhaul your entire library at once. Start with one brand and one clear objective.
- Phase 1 (Weeks 0–2): Review UCPMP guardrails and set up DPDPA consent flows. Identify your "Approved Claims Pack"—the science that cannot be altered.
- Phase 2 (Weeks 3–4): Pick a use case (e.g., Conference Follow-up). Create a "Master Template" in Studio by TrueFan AI.
- Phase 3 (Weeks 5–8): Distribute to a test group of 100 HCPs via WhatsApp. Monitor where they drop off.
- Phase 4 (Weeks 9–12): Compare the "Meeting Booking Rate" of the video group vs. a control group. Aim for a 20-30% lift.
Why Studio by TrueFan AI?
Medical data requires enterprise-grade security, not tools meant for social media creators. Studio by TrueFan AI offers:
- Consent-First Model: No video renders without a verified consent ID.
- MLR-Locked Templates: Medical teams lock safety data; marketing only changes the greeting and language.
- ISO 27001 & SOC 2: Meets the highest global and Indian data standards.
- Multi-Language Synthesis: Accurate lip-syncing so the doctor feels spoken to directly, not watching a dubbed clip.
- WhatsApp Integration: Generates unique, trackable links for high-open-rate environments.
Common Pitfalls
The "Creepy" Factor: Personalization should feel helpful, not like surveillance.
Bad: "I saw you were on our website at 2 AM, Dr. Sharma."
Good: "Dr. Sharma, since you recently requested info on [Drug X], here is the specific dosing guide for pediatric use."
The "Broken Link" Disaster: If a video buffers for 30 seconds, you’ve lost them.
Fix: Use adaptive bitrate streaming for instant play, even on 3G.
The "Compliance Lag": Waiting weeks for MLR approval on every variant.
Fix: Approve the template and the logic. If the "Claims Block" is locked, the system only needs to be approved once.
The Path Forward
The future of doctor engagement isn't about the biggest production budget; it’s about the most efficient data-to-video pipeline. By 2027, companies still relying on generic PDFs and 60-minute invites will be locked out of the doctor’s office. The winners will be those who respected the doctor's time and spoke their language.
Start small. Build your first module. Prove it works. Then, scale the trust.
Frequently Asked Questions
Does UCPMP 2024 allow us to mention the doctor's name?
Yes. Personalized greetings are professional communication, not "inducements." Just ensure the content remains strictly educational.
How do we handle opt-outs?
Under DPDPA 2023, you must provide an "Easy Opt-Out." Every landing page needs a clear "Unsubscribe" button that instantly stops variant generation for that ID.
Can we use AI avatars?
Yes, but transparency is key. For high-science content, using a "digital twin" of a real MSL or KOL (with permission) carries more authority.
Is WhatsApp compliant for clinical data?
It is the primary tool for Indian HCPs. To stay compliant, use the WhatsApp Business API and ensure links lead to secure, encrypted pages with full prescribing information.
What is the cost-per-doctor?
While setup has a cost, the "per-variant" cost is negligible compared to a failed rep visit. Most enterprises see a 40-50% reduction in production costs via modular automation.